Fabrizio Bartoletti, born in Bologna on 27 August 1576, at the same time as he studied philosophy, graduated in medicine on 26 March 1613 and took up the chair of logic at the University of Bologna in the same year, to then obtain that of anatomy in 1616. From 1620 to 1625 he will hold the chair of ordinary practical medicine, preserving also the right to teach anatomy, until Duke Ferdinando Gonzaga, having learned of his qualities and of his preparation, does not call him to himself to entrust him with the same roles in the nascent University of Mantua. After five years, having consolidated his position in the university thanks also to the esteem of Ferdinand’s successors, he will have to leave the city of Mantua, upset by the succession war and close to the siege of the imperial armies. Bartoletti will then return to Bologna, finding his death in Lendinara on 30 March 1630. Although he did not have time to learn about the discovery of blood circulation, he was a careful doctor who knew how to calibrate the Galenic dogmatism to the taste for Galilean observation, a supporter of that new clinical method that combined the examination of the patient with the anatomopathological dissection as well as chemist able to discover milk sugar.
The main medical work is the “Methodus in Dyspnoeam”, which appeared posthumously in 1632 but probably ended before 1628, a treatise in which Bartoletti attempts a rational classification of disturbances related to rhythm and depth of breath, starting from the belief that breathing was the means of bringing to the blood, through the air mixed with it, a quid which gave rise to the vital spirit which, in the brain, changed into the excitatory animal spirit, through nerves, organs and different limbs.
Bartoletti distinguishes four main classes of sick breath:
– deep and rare breathing, typical of the febrile delirium and due to the serious alteration of the regulatory centers of life;
– frequent and superficial breathing, in relation to an altered thoracic mechanics. It occurs in parietal pain in inflammations of the upper airways, in diaphragmatic and hypochondriac pain of an inflammatory nature, in deformation of the rib cage, etc.
– deep and frequent breathing, associated with altered lung mechanics. It occurs in the anatomical lesions of the lungs, in the pericardial sinchiae, in thoracic effusions, in the occlusions of the pulmonary arteries,
– rare and superficial breathing, connected with hysteria, apoplexy and other forms of cerebral weakness.
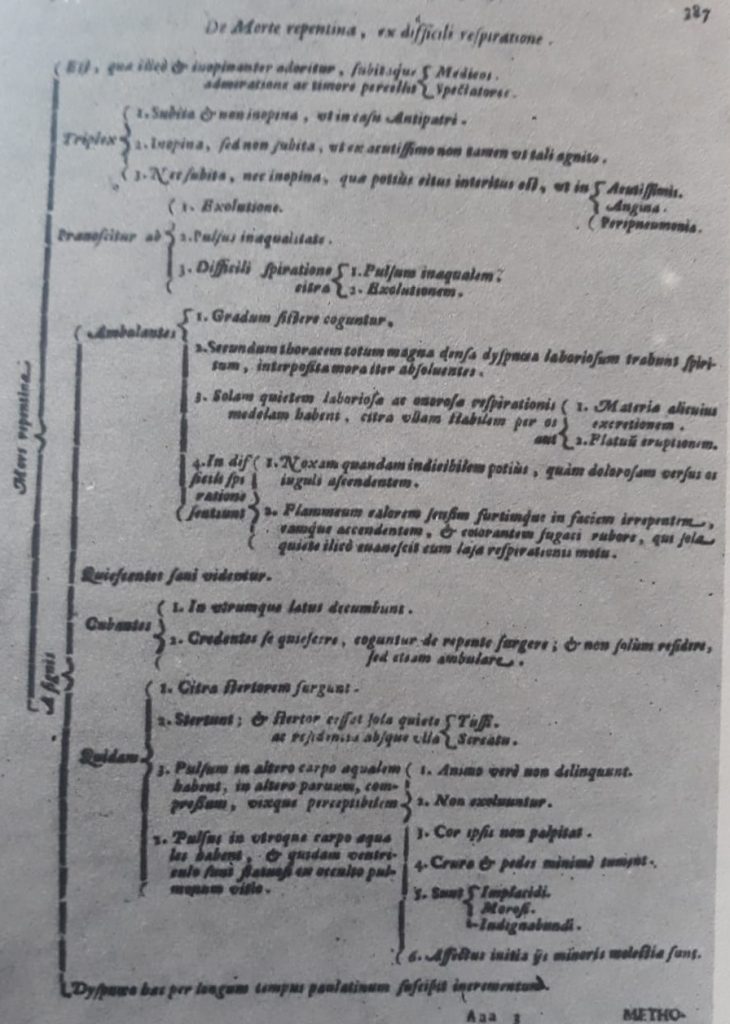
This treatise on functional respiratory pathology remained unsurpassed for more than two hundred years, with the remarkable merit of being the first to distinguish respiratory alterations in organic and functional. In the most salient passage of the entire volume, Bartoletti addresses the interactions of the breath that predict a sudden death and it is more than recognizable a good description of the angina pectoris of one hundred and fifty years prior to the classic description of Heberden. In the aforementioned passage, the Bolognese physician presents several cases of patients whose symptoms and conditions he noted and concludes that there is a sort of sudden death that often occurs but that is often omitted and that seems to have a difficult symptom as the only obvious symptom breathing, which is why many doctors do not even think of it as the only omen of imminent death. These patients have no fainting or syncopation or palpitations of the heart, they frequently see intervals in which they experience minor or no discomfort and because of them they are deceived and underestimate the only symptom that could explain their suffered condition. The anginal syndrome, in this note of Bartoletti’s text, is crystallized in its general lines: the sick are caught by a particular anxiety in the case of walking, even of brief entity, so as to be forced to stop or even to sit, any malaise disappears with the quiet of the person alone, there are no signs of circulatory deficiency such as irregular pulse, slack edema or hypnotic garden decubitus, in conditions of tranquility and absence of effort appear healthy, and, nevertheless, die of sudden death.
Differences are found with Heberden’s description, only in the presentation of the sensations that sufferers feel during the manifestation of the respiratory alteration. According to Bartoletti the evil would consist in a peculiar perception of breathlessness, while, in the opinion of the English doctor, access would be associated with a sense of strangulation and anxiety, without difficulty in breathing. This discrepancy can only depend on the different ways of considering and describing this symptom, since both refer to an identical phenomenon that compares to the annoying feeling of oppression experienced by those who travel a long and steep climb. It should also be emphasized that there is another slight difference, between the two scholars, and it is with regard to the irradiation of pain or the disturbing sensation, which according to Heberben from the sternum is transmitted to the left arm, while according to Bartoletti it reaches the clavicle.
A curious note can be found in the conviction, shared by both, that the cause of the illness could reside in the lungs and not in the heart, a possibility they did not mention.